
Bone Bruise – Wie viel Aufmerksamkeit ist dem blauen Fleck im Knochen zu schenken?
Mehr als nur ein blauer Fleck
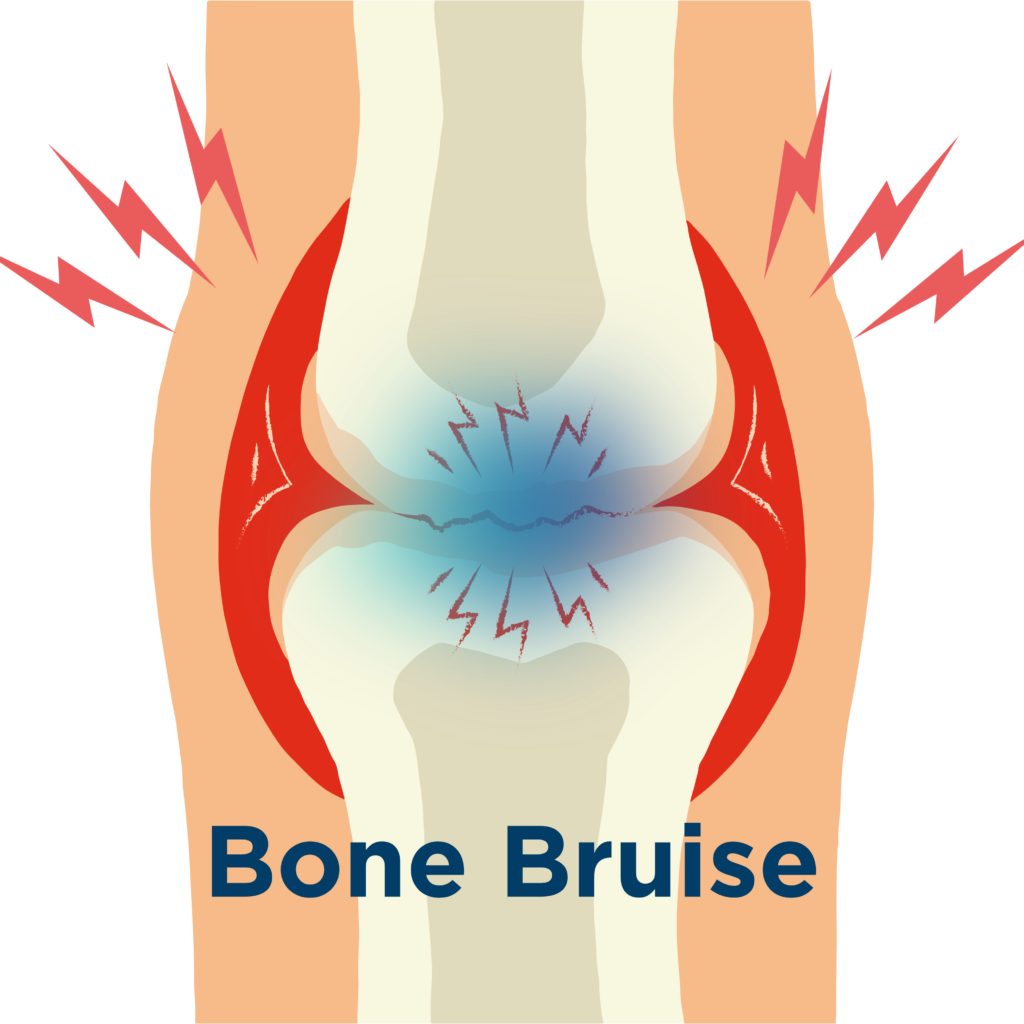
Ein „Bone Bruise“ klingt zunächst harmlos – schließlich denken die meisten an einen gewöhnlichen blauen Fleck. Doch genau hier beginnt das Missverständnis: Während ein klassisches Hämatom oberflächlich im Gewebe entsteht, liegt der Bone Bruise tief im Knochen verborgen. Es handelt sich um eine Verletzung mit Flüssigkeitseinlagerungen, Mikrotraumata und strukturellen Veränderungen im Knocheninneren.
Diese Verletzung bleibt im Röntgenbild oft unsichtbar und wird meist erst durch ein MRT erkannt. Genau das macht sie tückisch: Unsichtbar bedeutet nicht harmlos.
Entstehung: Wenn Belastung unter die Oberfläche geht
Bone Bruises entstehen in der Regel durch direkte Gewalteinwirkung, Kompression oder wiederholte Überlastung. Typische Szenarien sind Sportverletzungen, Stürze oder chronische Fehlbelastungen.
Im Inneren des Knochens kommt es dabei zu kleinen Gefäßverletzungen, Einblutungen und Ödemen – vergleichbar mit einem „inneren Bluterguss“. Anders als bei oberflächlichen Hämatomen betrifft dies jedoch die tragende Struktur des Knochens.
Symptome: Warum der Schmerz oft unterschätzt wird
Ein Bone Bruise äußert sich meist durch belastungsabhängige Schmerzen, die nicht sofort eindeutig zuzuordnen sind. Häufig verschwindet der erste Schmerz nach dem Trauma schnell – nur um später stärker und anhaltender zurückzukehren.
Genau diese zeitverzögerte Symptomatik führt dazu, dass Betroffene die Verletzung unterschätzen oder zu früh wieder belasten – ein kritischer Fehler.
Heilungsverlauf: Geduld statt Schnelllösung
Während ein klassischer blauer Fleck oft innerhalb weniger Wochen abheilt, kann ein Bone Bruise deutlich länger bestehen. Die Dauer reicht – abhängig von Schwere und Belastung – von mehreren Wochen bis hin zu Monaten.
Das Problem: Die Heilung verläuft nicht linear. Schmerzen können schwanken, Belastbarkeit täuschen und Fortschritte plötzlich stagnieren.
Risiko: Wann aus „harmlos“ problematisch wird
In vielen Fällen heilt ein Bone Bruise folgenlos aus. Doch wird die Verletzung ignoriert oder zu früh belastet, können Komplikationen entstehen. Dazu zählen strukturelle Schwächungen des Knochens oder im Extremfall die Entwicklung einer Stressfraktur.
Die entscheidende Frage lautet also nicht, ob ein Bone Bruise gefährlich ist – sondern wie man damit umgeht.
Fazit: Aufmerksamkeit ist kein Luxus, sondern Strategie
Ein Bone Bruise ist kein klassischer „blauer Fleck“, sondern eine ernstzunehmende Knochenverletzung mit oft unterschätzter Dynamik. Wer ihn ignoriert, riskiert einen deutlich längeren Heilungsverlauf oder Folgeschäden.
Doch hier wird es spannend:
Die eigentliche Herausforderung liegt nicht in der Diagnose – sondern in der richtigen Belastungssteuerung während der Heilung.
Denn genau hier entscheidet sich, ob du in wenigen Wochen zurück bist … oder monatelang ausgebremst wirst.
Dein DK Sports & Physio Team aus der Karlsruher Oststadt
Den ausführlichen Artikel findest du in unserer DK Academy.
Wir geben Physiotherapeuten, Trainern und allen Wissbegierigen einen sachlichen Einblick in die Physiotherapie und helfen so die Rehabilitation und das Training nach Verletzungen oder Beschwerden effizienter zu gestalten.
Sichere dir vollen Zugriff auf unsere Rehab Live Sessions, exklusive Review- und Blogartikel, Simple Tipps und Infografiken.

Du benötigst Physiotherapie im Raum Karlsruhe? Dann sind wir gerne für dich da und unterstützen dich!
Dein DK Sports & Physio Team aus der Karlsruher Oststadt
Unsere weiteren Blog-Artikel
Rotator cuff related shoulder pain – was steckt dahinter?
Hals über Kopf ins Märchen: Wer hat Angst vorm Handynacken?
Plantarfasziitis oder Plantarfasziopathie – Ursachen und Lösungen bei Fersenschmerzen

Vorsicht, piekst ein bisschen! Die Evidenz hinter Dry Needling
Was ist eine Arthrofibrose und was kann man dagegen tun?

Schmerzen erklären? Für Physios (k)ein großes Problem!

Osgood-Schlatter: Wenn Wachstumsschmerzen den Sport ausbremsen
Quellenangaben:
[1] D. B. Hoffmann, W. Lehmann, und S. Sehmisch, „Traumatic bone bruise“, Osteologie, Bd. 26, S. 96–99, Jan. 2017.
[2] P. Ward, P. Chang, L. Radtke, und R. H. Brophy, „Clinical Implications of Bone Bruise Patterns Accompanying Anterior Cruciate Ligament Tears“, Sports Health Multidiscip. Approach, Bd. 14, Nr. 4, S. 585–591, Juli 2022, doi: 10.1177/19417381211029583.
[3] C. Rangger, H. Goost, K. Kabir, und C. Burger, „Bone bruise: Morphologische Veränderungen und klinische Relevanz“, Trauma Berufskrankh., Bd. 8, Nr. S02, S. S178–S181, Aug. 2006, doi: 10.1007/s10039-006-1134-y.
[4] S. Sohn, S. M. AlShammari, B. J. Hwang, und M. S. Kim, „A Systematic Review of Bone Bruise Patterns following Acute Anterior Cruciate Ligament Tears: Insights into the Mechanism of Injury“, Bioengineering, Bd. 11, Nr. 4, S. 396, Apr. 2024, doi: 10.3390/bioengineering11040396.
[5] T. G. Sanders, M. A. Medynski, J. F. Feller, und K. W. Lawhorn, „Bone Contusion Patterns of the Knee at MR Imaging: Footprint of the Mechanism of Injury“, RadioGraphics, Bd. 20, Nr. suppl_1, S. S135–S151, Okt. 2000, doi: 10.1148/radiographics.20.suppl_1.g00oc19s135.
[6] R. Dai u. a., „Comparison of Bone Bruise Pattern Epidemiology between Anterior Cruciate Ligament Rupture and Patellar Dislocation Patients—Implications of Injury Mechanism“, Bioengineering, Bd. 10, Nr. 12, S. 1366, Nov. 2023, doi: 10.3390/bioengineering10121366.
[7] S. A. Patel, J. Hageman, C. E. Quatman, S. C. Wordeman, und T. E. Hewett, „Prevalence and Location of Bone Bruises Associated with Anterior Cruciate Ligament Injury and Implications for Mechanism of Injury: A Systematic Review“, Sports Med., Bd. 44, Nr. 2, S. 281–293, Feb. 2014, doi: 10.1007/s40279-013-0116-z.
[8] V. Bordoni u. a., „Bone Bruise and Anterior Cruciate Ligament Tears: Presence, Distribution Pattern, and Associated Lesions in the Pediatric Population“, Am. J. Sports Med., Bd. 47, Nr. 13, S. 3181–3186, Nov. 2019, doi: 10.1177/0363546519872975.
[9] R. Compagnoni u. a., „Validation of a new topographic classification of bone marrow lesions in the knee: the six-letter system“, Knee Surg. Sports Traumatol. Arthrosc., Bd. 29, Nr. 2, S. 333–341, Feb. 2021, doi: 10.1007/s00167-020-05957-y.
[10] J. P. DeAngelis und K. P. Spindler, „Traumatic Bone Bruises in the Athlete’s Knee“, Sports Health Multidiscip. Approach, Bd. 2, Nr. 5, S. 398–402, Sep. 2010, doi: 10.1177/1941738110377745.
[11] J. B. Driban, S. Lohmander, und R. B. Frobell, „Posttraumatic Bone Marrow Lesion Volume and Knee Pain Within 4 Weeks After Anterior Cruciate Ligament Injury“, J. Athl. Train., Bd. 52, Nr. 6, S. 575–580, Juni 2017, doi: 10.4085/1062-6050-52.1.09.
[12] P. Szaro, M. Geijer, und N. Solidakis, „Traumatic and non-traumatic bone marrow edema in ankle MRI: a pictorial essay“, Insights Imaging, Bd. 11, Nr. 1, S. 97, Dez. 2020, doi: 10.1186/s13244-020-00900-8.
[13] M. M. Chau u. a., „Osteochondritis Dissecans: Current Understanding of Epidemiology, Etiology, Management, and Outcomes“, J. Bone Jt. Surg., Bd. 103, Nr. 12, S. 1132–1151, Juni 2021, doi: 10.2106/JBJS.20.01399.
[14] J. M. Farmer, D. F. Martin, C. A. Boles, und W. W. Curl, „CHONDRAL AND OSTEOCHONDRAL INJURIES“, Clin. Sports Med., Bd. 20, Nr. 2, S. 299–320, Apr. 2001, doi: 10.1016/S0278-5919(05)70308-2.
[15] U. G. Longo, M. Loppini, G. Romeo, C. N. Van Dijk, N. Maffulli, und V. Denaro, „Bone bruises associated with acute ankle ligament injury: do they need treatment?“, Knee Surg. Sports Traumatol. Arthrosc., Bd. 21, Nr. 6, S. 1261–1268, Juni 2013, doi: 10.1007/s00167-013-2383-5.
[16] J. Moran u. a., „Examining the Distribution of Bone Bruise Patterns in Contact and Noncontact Acute Anterior Cruciate Ligament Injuries“, Am. J. Sports Med., Bd. 51, Nr. 5, S. 1155–1161, Apr. 2023, doi: 10.1177/03635465231159899.
[17] H. Shi u. a., „Bone Bruise Distribution Patterns After Acute Anterior Cruciate Ligament Ruptures: Implications for the Injury Mechanism“, Orthop. J. Sports Med., Bd. 8, Nr. 4, S. 232596712091116, Apr. 2020, doi: 10.1177/2325967120911162.
[18] H.-D. Wang, J. Zhang, Y. Li, Z. Li, W. Yan, und Y. Ao, „Classification of Bone Bruises in Pediatric Patients With Anterior Cruciate Ligament Injuries“, Orthop. J. Sports Med., Bd. 11, Nr. 2, S. 23259671221144780, Feb. 2023, doi: 10.1177/23259671221144780.
[19] J. V. Novaretti u. a., „Bone Bruise Patterns in Skeletally Immature Patients With Anterior Cruciate Ligament Injury: Shock-Absorbing Function of the Physis“, Am. J. Sports Med., Bd. 46, Nr. 9, S. 2128–2132, Juli 2018, doi: 10.1177/0363546518777247.
[20] J. S. Green u. a., „Posteromedial tibial plateau bone bruises are associated with medial meniscal ramp lesions in patients with concomitant anterior cruciate ligament ruptures: a systematic review & meta-analysis“, Phys. Sportsmed., Bd. 51, Nr. 6, S. 531–538, Nov. 2023, doi: 10.1080/00913847.2022.2108350.
[21] C. P. Helito, P. V. P. Helito, R. V. Leão, M. K. Demange, und M. Bordalo-Rodrigues, „Anterolateral ligament abnormalities are associated with peripheral ligament and osseous injuries in acute ruptures of the anterior cruciate ligament“, Knee Surg. Sports Traumatol. Arthrosc., Bd. 25, Nr. 4, S. 1140–1148, Apr. 2017, doi: 10.1007/s00167-017-4498-6.
[22] C. P. Helito, P. V. P. Helito, H. P. Costa, M. K. Demange, und M. Bordalo-Rodrigues, „Assessment of the Anterolateral Ligament of the Knee by Magnetic Resonance Imaging in Acute Injuries of the Anterior Cruciate Ligament“, Arthrosc. J. Arthrosc. Relat. Surg., Bd. 33, Nr. 1, S. 140–146, Jan. 2017, doi: 10.1016/j.arthro.2016.05.009.
[23] L. Lintin u. a., „The anterolateral ligament in acute knee trauma: patterns of injury on MR imaging“, Skeletal Radiol., Bd. 49, Nr. 11, S. 1765–1772, Nov. 2020, doi: 10.1007/s00256-020-03446-4.
[24] J. Moran u. a., „Injury to the Meniscofemoral Portion of the Deep MCL Is Associated with Medial Femoral Condyle Bone Marrow Edema in ACL Ruptures“, JBJS Open Access, Bd. 6, Nr. 4, Okt. 2021, doi: 10.2106/JBJS.OA.21.00069.
[26] H. Koiwai, M. Kamimura, A. Taguchi, K. Tensho, Y. Nakamura, und J. Takahashi, „Bone Bruises of the Ankle and Mid-foot Often Associate with Ankle Sprain“, 9. Oktober 2020, In Review. doi: 10.21203/rs.3.rs-68756/v1.
[27] G. Nishimura, M. Yamato, und M. Togawa, „Trabecular trauma of the talus and medial malleolus concurrent with lateral collateral ligamentous injuries of the ankle: evaluation with MR imaging“, Skeletal Radiol., Bd. 25, Nr. 1, S. 49–54, Jan. 1996, doi: 10.1007/s002560050031.
[28] Y. P. Khor und K. J. Tan, „The Anatomic Pattern of Injuries in Acute Inversion Ankle Sprains: A Magnetic Resonance Imaging Study“, Orthop. J. Sports Med., Bd. 1, Nr. 7, S. 2325967113517078, Dez. 2013, doi: 10.1177/2325967113517078.
[29] M. Randell, D. Marsland, E. Ballard, B. Forster, und M. Lutz, „MRI for high ankle sprains with an unstable syndesmosis: posterior malleolus bone oedema is common and time to scan matters“, Knee Surg. Sports Traumatol. Arthrosc., Bd. 27, Nr. 9, S. 2890–2897, Sep. 2019, doi: 10.1007/s00167-019-05581-5.
[30] A. Lutz, „Bone Bruise und Stressfraktur: Knochen im Stress | Symptome & Therapie“, Deutsche Zeitschrift für Sportmedizin. Zugegriffen: 16. September 2024. [Online]. Verfügbar unter: https://www.zeitschrift-sportmedizin.de/bone-bruise-und-stressfraktur-knochen-im-stress/
[31] C. Galloway u. a., „Relationship Between Bone Bruise Volume and Patient Outcomes After ACL Reconstruction“, Orthop. J. Sports Med., Bd. 11, Nr. 2, S. 23259671221146205, Feb. 2023, doi: 10.1177/23259671221146205.
[32] S. A. Mirghasemi, E. Trepman, M. S. Sadeghi, N. Rahimi, und S. Rashidinia, „Bone Marrow Edema Syndrome in the Foot and Ankle“, Foot Ankle Int., Bd. 37, Nr. 12, S. 1364–1373, Dez. 2016, doi: 10.1177/1071100716664783.
[33] S. J. Warden, I. S. Davis, und M. Fredericson, „Management and Prevention of Bone Stress Injuries in Long-Distance Runners“, J. Orthop. Sports Phys. Ther., Bd. 44, Nr. 10, S. 749–765, Okt. 2014, doi: 10.2519/jospt.2014.5334.
[34] A. N. Ververidis, K. Paraskevopoulos, K. Tilkeridis, G. Riziotis, S. Tottas, und G. I. Drosos, „Surgical modalities for the management of bone marrow edema of the knee joint“, J. Orthop., Bd. 17, S. 30–37, Jan. 2020, doi: 10.1016/j.jor.2019.08.025.
[35] E. Villari, V. Digennaro, A. Panciera, R. Ferri, L. Benvenuti, und F. Cesare, „Bone marrow edema of the knee: a narrative review“, Arch. Orthop. Trauma Surg., Bd. 144, Nr. 5, S. 2305–2316, Apr. 2024, doi: 10.1007/s00402-024-05332-3.
[36] T. Bretlau, J. Tuxøe, L. Larsen, U. Jørgensen, H. S. Thomsen, und G. Lausten, „Bone bruise in the acutely injured knee“, Knee Surg. Sports Traumatol. Arthrosc., Bd. 10, Nr. 2, S. 96–101, März 2002, doi: 10.1007/s00167-001-0272-9.
[37] T. Hoenig, A. Tenforde, A. Hirschmüller, M. Cassel, T. Rolvien, und K. Hollander, „Bone stress injuries“, Dtsch. Z. Für Sportmed. J. Sports Med., Bd. 74, Nr. 2, S. 47–51, Feb. 2023, doi: 10.5960/dzsm.2023.555.
[38] R. A. Wayner u. a., „Epidemiology of Bone-Stress Injuries and Health Care Use in Pac-12 Cross-Country Athletes“, J. Athl. Train., Bd. 59, Nr. 6, S. 641–648, Juni 2024, doi: 10.4085/1062-6050-0089.23.
[39] T. Hoenig, A. S. Tenforde, A. Strahl, T. Rolvien, und K. Hollander, „Does Magnetic Resonance Imaging Grading Correlate With Return to Sports After Bone Stress Injuries? A Systematic Review and Meta-analysis“, Am. J. Sports Med., Bd. 50, Nr. 3, S. 834–844, März 2022, doi: 10.1177/0363546521993807.
[40] N. N. Kale, C. X. Wang, Victor. J. Wu, C. Miskimin, und M. K. Mulcahey, „Age and Female Sex Are Important Risk Factors for Stress Fractures: A Nationwide Database Analysis“, Sports Health Multidiscip. Approach, Bd. 14, Nr. 6, S. 805–811, Nov. 2022, doi: 10.1177/19417381221080440.